1. The project and its context
Addressing Obstacles to Success[1] was a two-year project that sought to address science achievement rates in applied-health undergraduate degree programmes at Waikato Institute of Technology (Wintec), with particular attention to Māori. Throughout their teaching careers, staff members at Wintec have heard many anecdotal stories about science being a “problem” for midwifery and nursing students. Research to inform retention strategies for Māori students studying midwifery at Wintec indicated that science was a potential barrier to their overall success (Gibson-van Marrewijk, 2005). Notwithstanding this anecdotal concern, the nature and extent of science as a “problem” for any student had not been systematically researched up to that point. A scoping research project explored the following questions: Is science a problem? Is science the problem? Is science the only problem in the undergraduate applied-health programmes? (Gibson et al., 2005). The research found that many students experienced science as a difficult and time-consuming subject, and often prioritised study for science over other papers and assessment tasks. Furthermore, the research indicated that science was experienced as a difficult subject for all students, not just Māori students (Gibson et al., 2005).
In an area with a large Māori population, it is of particular importance that Māori students are supported to achieve success in becoming midwives and nurses who can proactively contribute to the care of their own people. Wintec is a Tertiary Education Institution (TEI) that is committed to Te Tiriti o Waitangi and local iwi. The TEI is situated in a region with a high density of Māori— 21 percent of people in the Waikato Regional Council area are Māori (Statistics New Zealand, 2006)—and Wintec provides qualifications in a variety of applied industry-focused areas, including targeted kaupapa Māori courses that reflect the aspirations and learning needs of the Māori community. Wintec has been proactive in developing courses that encourage wider participation of Māori within the tertiary learning arena. These include courses in te reo me ngā tikanga, and kaupapa Māori bridging courses to assist Māori to meet entry requirements into programmes across the institution. This project initially sought to focus on success for Māori students, but in view of the scoping findings it was widened to include all first-year students in the Bachelor of Nursing (BN) and Bachelor of Midwifery (BM) programmes.
Science as a “problem” for midwifery and nursing students
The science education research literature suggests that the decontextualised nature of much science learning can be an obstacle to many learners, especially when their world views do not mesh comfortably with those of the Western European culture in which science is based. For such learners, it may be necessary to create explicit “border crossing” strategies so that they come to understand this mismatch and make the necessary translations between the differing world views (Aikenhead, 1996). Another obstacle is that science ideas are often expressed in formal, abstract, logico-scientific modes of communication, whereas people mostly use more informal and storied narrative modes of communication (Bruner, 1986). It takes practice and careful support to learn to use these new modes, and learners may not see a need to make this effort unless they can see an identity for themselves as learners and users of science knowledge (Gilbert, Hipkins, & Cooper, 2005).
Research into the use of science knowledge in science-based occupations highlights another set of related dilemmas. Such research has “produced one clear and consistent finding: most often, canonical scientific knowledge is not directly useable in science-related everyday situations [italics original], for various reasons” (Aikenhead, 2005, p. 245). One reason is that science is often “black boxed” in the technology used in workplace settings and therefore tends to be invisible in its application. Research suggests it is not recognisable in the form in which it is presented in science lessons, and students often don’t see the connection between what they learn in class and what they do on placement or might do in the future. Although this example comes from veterinary nursing, the problem is the same:
… the workplace science for understanding which bag to use on animals undergoing anaesthesia was limited to making sure that the animals can breathe correctly. It did not delve into the school science related to this topic with its reliance on calculations of total volume, tidal volume or residual volume, nor did it explore the mechanisms that control breathing. Within workplace science, declarative knowledge about sterilization was limited to knowing that the sterilization tablets changed to the appropriate colour to ensure that the surgical tools were sterile. The same concept with school science would focus on different kinds of bacteria, the structures that some bacteria have (i.e. endospore capsules) that make them resistant to heat and the required conditions necessary to kill such bacteria. (Chin, Munby, Hutchinson, Taylor, & Clark, 2004, p.129)
Aikenhead, along with others who have researched work settings, found that nurses are most likely to draw on their procedural knowledge when making decisions on the job—that is, their knowledge of what to do and how to do it. Nutley, Walter, and Davies (2003) point out that such procedural knowledge is likely to be tacit—that is, “you know how to do something but cannot readily articulate this knowledge” (p. 129). They contrast this type of knowledge with declarative knowledge—“knowledge that you can state”—which is what is more likely to be taught and assessed in science modules for midwifery and nursing. They suggest that there is a need to investigate “whether practice is more a case of ‘from doing to knowing’ (the social construction of knowledge) rather than ‘from knowing to doing’ (rational EBPP [2] models)” (Nutley, Walter, & Davies, 2003, p. 129). Of course, procedural knowledge is not unrelated to declarative knowledge. As Aikenhead (2005) points out:
… there is a relationship between scientific knowledge and professional knowledge of nursing. Some professional content used today was certainly developed as a result of the deconstruction and reconstruction of scientific concepts in a context of specific interest to most nurses, but it would not be recognised in its present form as legitimate science content to a science instructor [italics added]. (p. 271)
In light of findings such as these, helping students to see clearer connections between their science learning and their goal of becoming midwives or nurses became central to our project.
The research sought to find ways to support students to make links between theory and practice. We anticipated that this would require a change from traditional teaching, which tends to leave students to create links for themselves. The overall thrust of the research is summarised in the following diagram.
A shift from traditional teaching:
Figure 1 The type of change to traditional teaching sought by this research

To this model:

Undergraduate midwifery and nursing education
The Midwifery Council of New Zealand and the Nursing Council of New Zealand are the statutory authorities responsible for setting and monitoring standards for registration. They provide guidelines for nursing and midwifery education; administer state examinations; and receive applications for registration. TEIs in New Zealand develop curricula based on the midwifery and nursing councils’ guidelines for education, including broad principles for the inclusion of science in degree programmes and for standards of practice/competencies. It is important to state that our project did not seek tochallenge the guidelines, but rather to help student midwives and nurses overcome obstacles to success in learning the science prescribed.
Through its School of Health, Wintec is one of five New Zealand TEIs that teach both the BM and the BN undergraduate degree programmes. Eleven TEIs teach only the BN.
The School of Health has an average annual intake of between 160 and 200 students, of whom 25–40 (20 percent) identify as Māori (Wintec, 2004). Wintec is the only TEI that offers a specific support programme for Māori students in applied-health programmes, Tihei Mauri Ora (TMO). Māori students have the option to enrol as either a mainstream student or into Tihei Mauri Ora, whose special character is explained as follows:
The Tihei Mauri Ora option integrates all pertinent areas of knowledge from both the Western and Māori worlds. It recognises the potential within a Māori paradigm and begins to address the needs of a minority community who are partners with non Māori. It supports the pertinent articles of the Treaty of Waitangi … by implementation of a body of knowledge that is explicitly Māori. From this platform, we have been able to embrace a greater sensitivity to cultural diversity in a broader context as well. (Wintec, 2007a)
The three-year full-time undergraduate degree programmes at Wintec are taught by midwifery and nursing tutors, with the exception of the science modules, which are taught by tutors from the School of Science and Primary Industries.
2. Overall research design
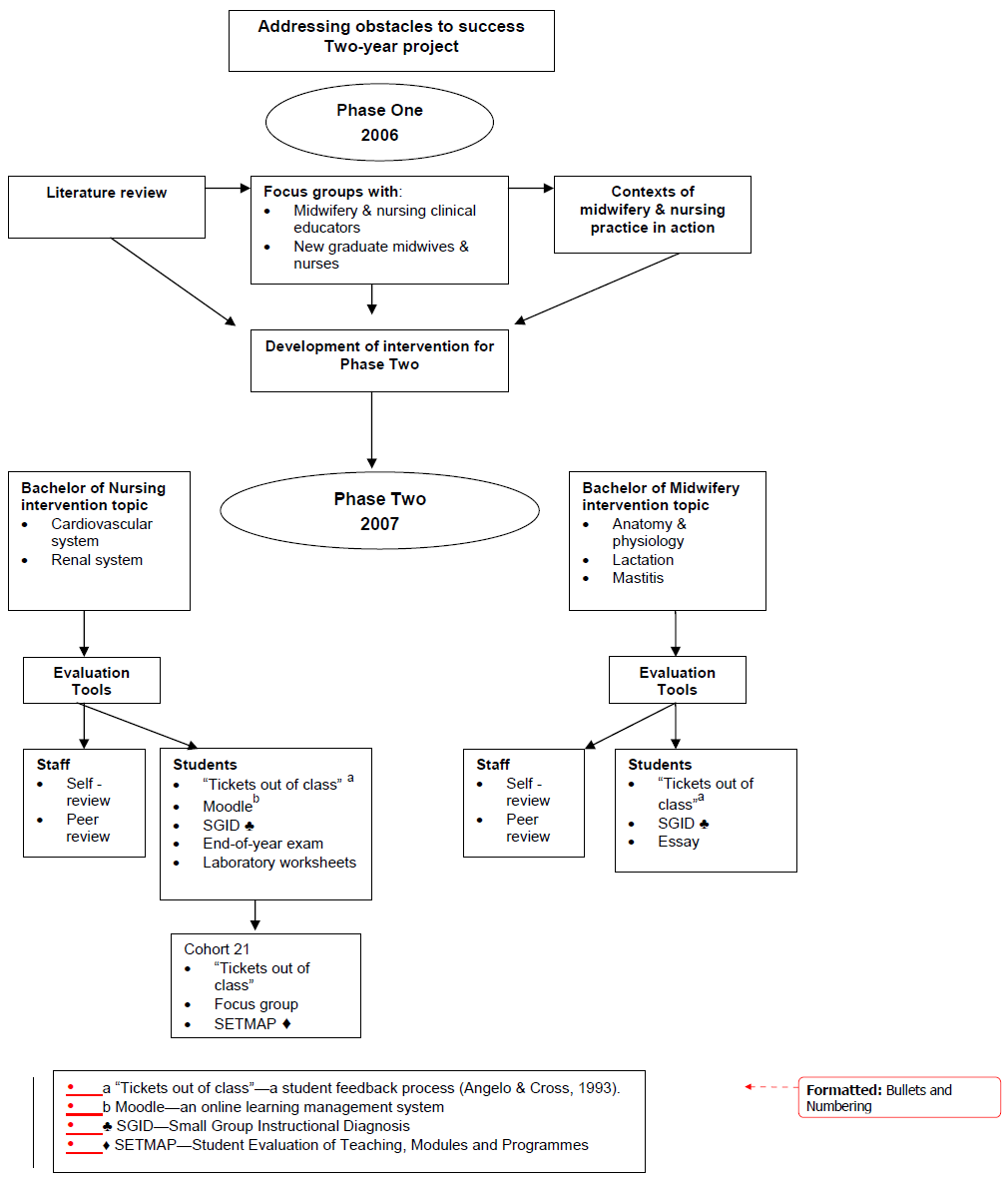
This research project aimed to find new ways to include the necessary science knowledge in undergraduate degree programmes for midwifery and nursing without making this an obstacle to overall programme success. The research comprised two phases which are summarised in Figure 3.
Phase One (2006) sought to answer the question: “What aspects of science do newly graduated midwives and nurses really need to know in order to practise competently?” Activities at this stage included:
- a review of current literature to identify findings of relevance from science education for applied health programmes
- focus groups with midwifery and nurse educators, and new graduate[3] midwives and nurses, to explore the science they see as actually used in practice.
The findings from Phase One assisted us with planning and developing an intervention for Phase Two.
Phase Two (2007) sought to answer the question “How can science be taught more effectively to help students make more meaningful theory–practice links?” by:
- designing, delivering, and evaluating the effectiveness of a pilot intervention in two subject areas of the BN science module, based on the “essential” science knowledge and skills identified in Phase One, and matched to aspects of the current curriculum being taught
- designing and delivering a breastfeeding and lactation module, taught primarily by midwives, but with science (taught by science tutors) integrated into the module.
The use of narrative as a pedagogical strategy for interweaving theory and practice was central to the intervention. Narratives were designed for four lectures in a module on lactation and breastfeeding for first-year midwifery students, and for two topics—cardiovascular system and renal system (three lectures each)—in the science module for first-year nursing students. The short, focused narratives were designed to put the theoretical ideas and the contexts of life and work into closer juxtaposition. In the nursing science module, where the science tutors had more control over the whole curriculum, other changes were also made. These are described in more detail later in the report.
Figure 2 A summary of the research activities and data sources
Cohort 21
Most of the participating BN students (n=160) were in their first year of the degree programme. We were particularly interested in one group of students—called Cohort 21 (n=21) who were nursing students repeating first-year science, having failed it the first time. They attended the same lectures but completed their science laboratories as a separate group from the first-time students. Since Cohort 21 first undertook science in 2006, when there were no research interventions in the module, and they would be undertaking science in 2007 when interventions were being introduced in two subject areas, we thought that it might be useful to capture any comparison information through the data collected.
We asked the Cohort 21 students to compare 2006 and 2007 in the following areas: what helped their learning; what hindered their learning; suggestions for improvement; and whether the impact of clinical practice in 2006 helped/hindered learning in relation to the cardiovascular system and the renal system interventions in 2007. This final question was of particular interest because Cohort 21 students were the only ones with some exposure to the practical side of their nursing training before commencing the science module. We anticipated that gathering information about the links these students made between their prior experiences/knowledge and the science theory they were relearning in 2007, presented in a slightly different way, could provide useful insights into the challenges of translating theory to practice that we were seeking to address.
In the event, as we later describe, this group contributed less to the overall findings than did the mainstream students.
3. The research as it unfolded
Phase One addressed the question “What science do newly graduated midwives and nurses really need to know in order to practise competently?” The overall aim of the first phase was to collect data from “expert” midwifery and nurse educators and new graduate midwives and nurses in order to tap into their “know-how” and build narratives for use in the science classroom.
The literature highlighted the importance of contextualising science education by making the links to workplace practice more explicit. The literature is critical of traditional teaching that leaves students to make the translation between theory and practice, as shown in Figure 4.
Figure 3 The traditional siutation—tacit links between science learnt and practised

However, before we could address the challenge of changing this situation, we needed to explore the science that midwives and nurses actually used in practice. The initial literature search also suggested that encouraging our professional participants to see the tacit connections between their practice and the underpinning science would require careful attention to the design of the research instruments for the first phase. Using a narrative approach (Aikenhead, 2005; Benner, 2001) provided a methodology for collecting rich contextual stories, which could be analysed in order to expose the underpinning science, as well as potentially providing us with a source of stories for the second phase of the research.
The focus groups
Fourteen regionally based focus groups were held with participants from three TEIs and three District Health Boards. These collected perspectives from midwifery and nurse educators, and new graduate midwives and nurses, about their work and its perceived science–practice links. Almost all of the 80 participants were female and identified themselves ethnically as New Zealand European. Despite our intention to create more diverse groups, only a small number identified as being ethnically New Zealand Māori or New Zealand Māori/New Zealand European. Consequently, two additional focus groups were held in one region, with Māori new-graduate midwives and Māori new-graduate nurses respectively.
Participants completed a brainstorming exercise in pairs or small groups. During this exercise they identified four to six aspects of their professional work relating to three key roles. These roles, shown in Table One, had been identifed by the research team during preparation for the field work and were given as a starting point for discussion.
| Key midwifery roles | Key nursing roles | ||
|---|---|---|---|
| A. | Working in partnership with women to provide the necessary support, care, and advice during
|
A. | Caring for the physical condition of the patient, enhancing their state of health/healing |
| B. | Being responsible for the birth and care of the newborn | B. | Attending to, and supporting, the patient’s emotional well-being and physical comfort |
| C. | Providing health counselling and education, not only for the woman, but also the family and community | C. | Acting as a go-between for the patient and other people (doctors, other medical specialists, family members, etc.) |
Following this brainstorming exercise, focus-group facilitators asked participants to discuss and record examples of practice for each role. This provided us with an opportunity to capture narratives of practice for subsequent analysis. The common themes which emerged are outlined further in this report.
The session was completed with a final question for each pair/small group—“How do you think the science learnt/taught during the midwifery/nursing programme contributes to these key aspects of your work?” Participants found this question difficult to answer and could not identify the science underpinning the tasks they complete. This was a vivid illustration of the difficulty of translating science into practice, highlighted in the science education literature.
Data analysis—Identifying science used in practice
Data analysis involved several steps. Initially focus-group conversations were analysed in four categories so that we could look for differences in perspectives: new graduate midwives; midwifery educators; new graduate nurses; and nurse educators. Detailed notes, made by members of the research team during the focus groups, were the primary data source. These notes were supplemented by audio-taped records, which also served as a source of detailed quotes and a checking mechanism for accuracy. The diagrams participants completed in each small-group brainstorm were used to capture terminology and examples of “actions in practice”.
Analysis was undertaken collectively in a workshop setting. All the researchers who had taken part in focus groups came together to identify key themes from the accumulated materials. Data was recorded in a table format, with individual team members adding stories of practice that illustrated each of the emergent themes/subthemes. Table Two shows one example of the form the analysis took at this stage of the project.
| New graduate midwives | |
Theme
|
Stories of practice |
Education (Patient)
|
|
The science tutors then worked with the data to identify the specific science content underpinning the participant stories. This was added to the summary tables as a third column. Table Three shows this expansion of Table Two.
| New graduate midwives | ||
Theme
|
Stories of practice | Underpinning science Concepts |
Education (Patient)
|
|
|
In another workshop, the research team undertook a further round of analysis. This time the tabled data was used to identify rich contexts that could potentially be used to construct narrative materials for the classroom. For example, diabetes was identified as a “rich context” because it often came up in the stories told by both midwifery and nurse educators, and new graduate midwives and nurses. Rich contexts were recorded in summary tables and stories of practice were included. Again the science tutors then identified the underpinning science concepts in stories from each of the categories. Table Four shows one example.
| Nurse Educators | ||
| Rich content | Stories of practice | Underpinning science Concepts |
| Drugs—interaction of … | Entering into a relationship with a confused patient. What is the cause of the confusion—hypoxic/drug-related? | O2 exchange, hypoxia, drugs’ mode of action |
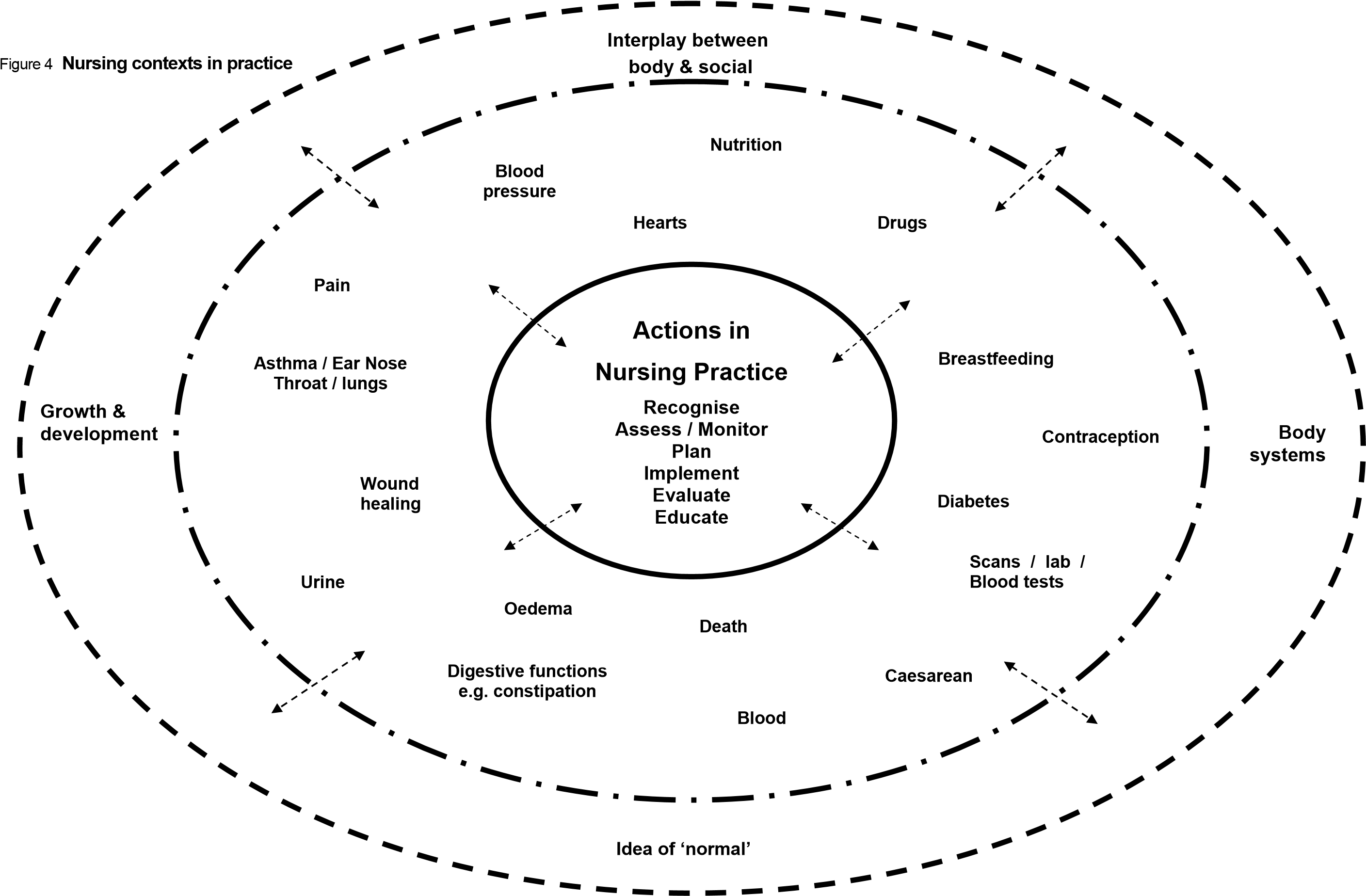
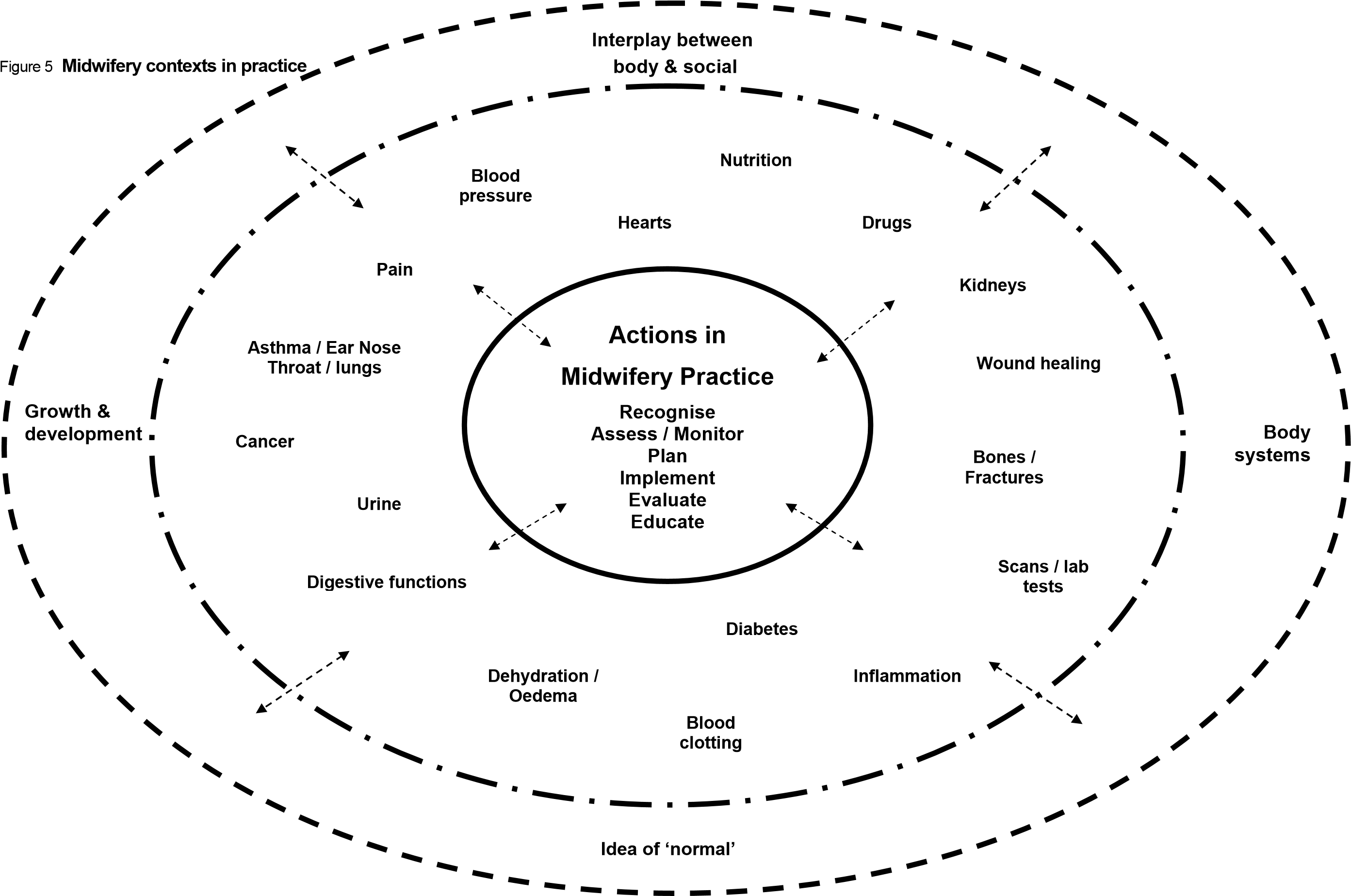
Following this second workshop, the four categories of participants were collapsed down to two areas—midwifery and nursing—because there were insufficient differences between the narratives of the less and more experienced practitioners to sustain the four categories. In fact, a core group of “actions in practice” emerged from the narratives. These included midwives and nurses being able to: recognise; assess/monitor; plan; implement; evaluate; and educate, albeit in sometimes differing professional contexts.
The researchers noted that metathemes were woven into all of the “actions in practice” and “contexts in practice”, and inter-relationships occurred between contexts. Metathemes identified by the researchers were:
- growth and development
- idea of ‘normal’/ranges of normal
- body systems
- interplay between the body and the social.
The interrelatedness of “actions in practice”, “contexts in practice”, and the metathemes were then shaped in diagrammatic form, as shown in Figures Five and Six. The circles represent the holistic nature of practice for midwives and nurses. The double-ended arrows represent the interlinking and interactions between “actions in practice” (central circle), “contexts in practice” (middle circle) and the metathemes (outermost circle).
Preparation for Phase Two
The findings from Phase One provided the basis for deciding on the content to be covered in the pilot intervention. Many of the examples of nursing practice related to aspects of the cardiovascular system—for example taking and recording blood pressure—or to aspects of the renal system—for example kidney failure or diabetes. Both these systems have traditionally been included in first-year science modules, and so they were chosen as intervention topics for the Bachelor of Nursing students. Each of the two science tutors taught one of these topics. The lactation and breastfeeding module was selected as the BM intervention. The midwifery team member and one of the science tutors had already planned to teach this module together, which presented an opportunity for an intervention that would not otherwise have been available.
It was intended that material from the first stage of analysis would provide a source of narratives that could be shaped as learning materials to link theory with practice in the intervention topics. These teaching stories could be used in lectures to make connections between the more abstract science and everyday experiences, as well as the (anticipated) professional work of midwifery and nursing, where relevant. In this way, it was hoped that students might see an identity for themselves as learners and users of the science knowledge being taught (Gilbert, Hipkins, & Cooper, 2005).
As it turned out, this translation process was not as straightforward as we had anticipated. All of the examples of practice from Phase One drew on concepts of un-wellness or “deviations from normal”. This was a mismatch with the existing first-year curriculum, in which the nursing science modules focused on wellness and normal body functioning. This had been a considered curriculum choice, made to ground students’ understanding in well-functioning contexts before they were exposed in the second year curriculum to the patho physiology of situations where medical intervention and nursing practice may be more directly implicated. The science tutors used considerable ingenuity to try and overcome this mismatch, developing stories that, while related to the rich contexts, drew on more familiar life contexts, albeit often implicating a need for medical intervention in the very near future! The following is an example:
New Zealand race-walker Craig Barrett collapsed during the last kilometre of the 50 km walk in the 1998 Commonwealth Games. He became confused and disorientated and staggered aimlessly before being removed from the race and successfully treated. (Wintec, 2007b)
The Craig Barrett narrative used in the renal topic provided a means to discuss “normal” and “not normal” with students, and provided a context for bringing everyday experience and prospective nursing experiences into the learning. For example, some questions were designed to generate discussion about what the renal system actually does for each of us when functioning correctly, and some about what nurses may really do:
Craig had been drinking during the race to prevent dehydration, but was he drinking water or “sports drinks”? Is the difference important? Did he drink too much, or not enough? How could you tell? How was he treated? (Wintec, 2007b)
Making space in the curriculum for the effective use of these stories was another challenge. The science tutors carried out a review of all the other materials they intended to use, with a view to content reduction. To support them in this challenging endeavour, the whole research team took part in extensive discussion regarding possible changes to the topics and how resources could be reshaped. This review was underpinned by principles of content reduction derived as part of a large-scale science education initiative called Project 2061 in the USA (American Association for the Advancement of Science, 2001). The team sought to: cut some topics; prune subtopics not essential to understanding; trim use of overly technical vocabulary; and reduce any unnecessary repetition.
Changes made to lectures included: the reduction of content and amount of detail in lectures; the revision of visual aids such as complex diagrams and introduction of more relevant examples in different mediums; the inclusion of narrative stories relating to the topic to establish relevance; adopting a strategy to get student feedback at the end of lectures; the revision of structure and content of corresponding laboratory sessions; and the introduction of diagnostic testing information. Staff aimed to increase the level of student interaction through online activities and in-class/laboratory discussion and activities.
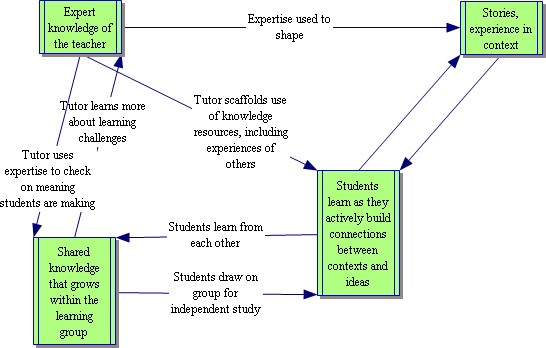
All these changes challenged the science tutors to rethink the ways they used their expertise to support the students’ learning. This rethinking of roles is summarised in the next figure, which stands in contrast to traditional teaching by “telling”.
Figure 6 Rethinking the use of subject expertise in teaching
4. Changing science teaching
Phase Two (2007) involved implementing and evaluating the effectiveness of the pilot intervention in one integrated module for first-year midwifery students and two topics in the science module for first-year nursing students. The “essential” science knowledge and skills identified from Phase One were matched to aspects of current curriculum being taught. Selected aspects of the module were then redesigned, bearing in mind the research imperative to explore ways to more meaningfully link theory to prospective professional practice. The redesign involved the contextualisation of science concepts to make stronger links to midwifery and nursing practice; content reduction to avoid overload; and use of activities that would draw students’ attention to the intended learning.
The changes in the Bachelor of Nursing science module (Semester 1, 2007)
First-year BN students are taught science in a full-year module. The two topics selected and developed as the intervention for the BN were the cardiovascular system (CVS) and the renal system. Each involved three classes over three weeks. These lecture classes had their existing content streamlined, narrative stories added (as already described), and a feedback process put in place. Some changes were made to accompanying laboratory worksheets to highlight the theory– practice links we hoped the students would build for themselves.
The feedback process involved the use of “tickets out of class” (TOC) (Angelo & Cross, 1993). At the completion of each lecture, students were invited to write on a slip of paper that prompted them to recall what they saw as the main idea of the lecture, and to ask any outstanding questions about the content of the lecture. Anonymous responses were posted into a box and reviewed by the science tutors. This strategy was seen as workable with a large class (approximately 160 nursing students). It provided opportunities to increase student participation and interactivity, and encouraged them to reflect on the intent of the lecture and on their own learning. The strategy also allowed the tutors to check the sense students had made of the theory and the narrative examples used in class. These insights provided useful feedback as the project unfolded.
In the BN science-for-nursing module, laboratory sessions supplement learning and provide students with a more detailed and practical application of some of the theory concepts covered in lectures. Students completed one laboratory for each intervention topic. The content of these sessions was revised in similar ways to the lectures, with content reduction and use of narrative materials. In some cases students’ attention was directed to a previously used narrative example, for instance:
Think back to the lecture story of Craig Barrett who collapsed during the 50 km walk at the Commonwealth games.
Do you think his problems were related to too little, or too much water?
Could you use body weight to determine whether he had drunk too little or too much water?
How much does a litre of water weigh?
What was the average increase in weight after drinking the water? (Wintec, 2007b)
A small number of additional questions were added to the existing laboratory session worksheets. These questions sought evidence that the students realised there were links between their science learning and their future role as nurses by asking them about ways the activities they had just carried out might align with the sorts of information nurses might contribute to patient’s care.
Evaluating the science-for-nursing intervention
A number of strategies were used to seek evidence of the impact of the changes in teaching approaches on students’ understanding of the science, their attitudes to the science module, and their ability to see links between the science and their prospective role as nurses. The evaluation sought evidence of impact from:
- students’ responses on the TOC
- their responses to the additional laboratory worksheet questions
- tutor self-review of teaching the intervention topics, and a peer interview with another research team member
- student feedback via an established group evaluation process called Small Group Instructional Diagnosis (SGID)[4]
- a routine end-of-module evaluation process, known at Wintec as a SETMAP[5]
- patterns of self-directed study using Moodle resources provided
- results from summative assessments undertaken by all students at the end of the module.
Cohort 21
- Students’ TOC responses to an additional question for the laboratories—“what aspects of today’s laboratory connect with clinical experience?” (CVS laboratory n=16, renal laboratory n=9);
- a focus group (n=3) where students were asked to compare learning for the intervention topics in 2007 with the same topics in 2006 regarding: what helped learning; what hindered learning; and suggestions for improvement—we also explored whether clinical practice in
2006 had helped or hindered learning in relation to the intervention topics in 2007 y a SETMAP comprising 20 Likert Scale questions developed by the research team to test some of our assumptions around teacher actions comprising questions about: content reduction; the inclusion of narratives; clinical practice and TOC; and around learner actions, comprising questions about revision/study; clinical practice; learning outcomes and laboratories; written feedback about aspects of the module that were done well; aspects in need of improvement; and any other comments (n=6).
The changes in the Bachelor of Midwifery breastfeeding and lactation module (Semester 2, 2007)
First-year BM students complete a breastfeeding and lactation module. The intervention for this module involved integrating and aligning science content into four classes: anatomy and physiology of the breast; lactation; composition of breast milk and physiology of infant sucking; mastitis, inflammation, and wound physiology. When lactation was discussed by the midwifery tutor, the relevant science for the anatomy and physiology of lactation was covered by the science tutor. The content for the science components was streamlined, a feedback process using TOC was implemented, and additional self-completion exercises for students were introduced.
One main narrative was used to link all four lectures. For this reason it was somewhat longer than those used in the first-year science classes outlined above.
Zoe was an 18-year-old primigravida [woman who is pregnant for first time] who was curious about the changes she observed in her breasts as her pregnancy progressed, and she had lots of questions for her midwife. She understood that pre-pregnancy breasts contained a lot of fat and wondered what happened to the fat as her breasts developed. Was fat replaced with glandular tissue? If so, does it come back? What proportion of her breasts are fat and what proportion mammary tissue when they are mature? What will happen to her breast after breastfeeding? Will they go back to the pre-pregnant size and shape?
As her breasts became larger Zoe noticed the appearance of blood vessels under the surface of the skin. She wondered if that was normal. Maybe they have just become more visible due to the skin changes or removal of fat? Also why were the nipples and areola getting darker in colour? She had also noticed that her breasts were tender and even quite painful at times. Why was that?
As she followed and learned about the changes in breast anatomy in preparation for breastfeeding, Zoe wondered about some of her friends. One of them has had a breast enhancement operation and another a reduction. Both had had their nipples pierced. Could any of these procedures cause damage that may affect breastfeeding? (Wintec, 2007c)
Evaluating the science-for-midwifery intervention
A number of strategies were used to seek evidence of the impact of the changes in teaching approaches on students’ understanding of the science, their attitudes to the science component of the midwifery lectures, and their ability to see links between the science and their prospective role as midwives. The evaluation sought evidence of impact from:
- students’ responses on the TOC
- tutor self-review of teaching the intervention topics and a peer interview with another research team member
- student feedback via SGID (n=27)
- a routine end-of-module evaluation process, known at Wintec as a SETMAP y results from a summative assessment essay.
For the essay, students interviewed one woman about breastfeeding and discussed the help which could be provided by professionals, the science underlying the process of lactation, and the rationale. With student permission, the research team accessed blind copies of the essay, so that they could review the science component of each student’s work.
Evidence of effectiveness of the intervention
Students’ engagement with the science
The feedback strategy (TOC) generated a range of questions about the topics covered in the lectures. In some instances students demonstrated that they were beginning to make links between theory and practice, prompted by the narratives the tutors had devised. For example, during one renal lecture on the topic of body fluids, one student asked:
How do you treat people that have too much water or too little water in their system, and how do you tell just by observing someone without weighing them?
Similarly, during a lecture about the composition of breast milk, two students asked:
What are the implications for a woman who may have overdosed herself on vitamin C meanwhile wanting to breastfeed? Are there any problems long term for mum & baby? Can mum breastfeed?
Is dopamine the same thing as prolactin inhibitory factor (PIF) or is there more than one type of PIF? If a lack of oxytocin to push milk into baby’s mouth—does manual breast compression work? Is breast compression harmful?
Students used the TOC to make positive comments about the manner in which the lectures were conducted. The extent of this positive feedback took one of the tutors by surprise but was affirming. By the end of the intervention this tutor said they were “feeling very positive about the intervention and will use the strategies for all my lectures from now on”.
Through the SGID feedback, students expressed appreciation at being able to ask questions and have a staff member available to answer their questions. TOC were also helpful because:
… in the next class the lecturer goes over the questions we may have had.
I do not cope very well with asking questions during class. I have a fear of humiliation. I suffer from extreme panic attacks where I can not and do not ask questions from the tutor in class. I responded well to the question cards (green) because I was able to write the question and gained an answer, this was much better for my learning.
Similarly, midwifery students commented that “being able to write questions and have them answered in the next lesson” and the fact that “lecturers always answer questions” helped their learning.
TOC was also viewed positively by the Cohort 21 students who were repeating the module. Their comments reflect similar themes to those made by the first-year student quoted above:
The tickets out of class helped me focus in class—explain in my own words on the ticket and the other portion with question—any doubt in understanding—did not have any fear because anonymous but my questions would have a forum in which to be addressed. You are giving feedback—never seen that before I think that it is great.
Tutors also recognised the value of using TOC with students. For example, one tutor said “I will consider using ‘tickets out of class’ on other occasions because it does give students the opportunity to ask questions when they may not in the big group.”
SGID feedback from BM students was that the integration of science with the midwifery content in the breastfeeding and lactation module helped with their learning. For example:
I think the science helps put everything into perspective.
Was definitely helpful having the science information available during the lactation class period.
Responding to the SETMAP, almost all students for both the BN and TMO groups agreed/strongly agreed that “teaching and learning resources for this module assisted my learning”. However, these responses also revealed that students were divided in their views about whether they “received prompt and regular feedback on their progress”. Of all the responding BN students (n=88), 19.32 percent strongly agreed, 36.36 percent agreed, and 28.41 percent were uncertain. These different responses may well reflect the extent to which students took an active part in the TOC process. The data does suggest that fewer students used TOC as the science module progressed. (The total number of BN students was 160, the average number of TOC responses for the CVS topic was 82 and for the renal topic was 45). It may be that, after the novelty wore off, students mainly used TOC when they had a specific question they wanted to have addressed.
Moodle is an online learning management system used by Wintec. The science tutors checked to see if online activity by BN students demonstrated increased engagement with science in the intervention topics. Five mini quizzes relevant to each of the BN interventions were chosen and the students’ engagement recorded and then correlated with their summative test scores. The results showed no significant correlation between the use of the formative quizzes and the summative test results. It was anticipated that the online activity report from 2007 would be able to be compared with online activity from 2006, however they could not be compared because of a change in the data programme used. Nevertheless, the impression that teaching staff have anecdotally is that there was an increase in the use of Moodle.
Evidence of emergent theory–practice links
From the SGID feedback, students said that using narrative examples or real-life examples had been helpful for learning when they took part. They said they understood better and the narratives helped put learning into context. For example, midwifery students commented that stories had helped their learning:
Being able to relate the information to us or people so the use of the story is great.
The story at the beginning—makes it more relevant to course, seems to help understanding and visualisation of issues talked about.
The science tutors reported that students seemed particularly interested, asking questions about the stories and often wanting to talk after the breastfeeding and lactation module lectures— students were engaged with learning despite the late-afternoon time slot for the class.
Few students seemed to grasp the thrust of the additional laboratory worksheet questions. For the first BN intervention topic most students simply repeated the information about what a pulse measures (81 percent of responses). Just 6 percent of the class (n=124) linked their role as a nurse to the context of pulse taking, even though this is a very common activity for a nurse to undertake. With varying degrees of specificity, these students did describe a connection between the nurses’ role and the information that could be gained from taking a pulse:
Whether this person is in good health or needs attention i.e. weak and thready might mean blood loss somewhere or shock?
A high pulse can be caused by presence of a fever or low pulse can = blood loss etc.
If the patient needs surveillance, looking after or medications.
May indicate underlying health issues that need further investigation.
If, as seems likely, unfamiliarity with the type of question being asked contributed to the low numbers answering along the lines anticipated, future students will need the link modelled for them the first time they encounter the format. This was a useful insight for the science tutors as they carried out self- and peer-reviews at the end of each intervention topic. Indeed, during the renal topic lecture on the kidneys/excretory system, more students did succeed in making the links being sought. Feedback during the earlier unit doubtless contributed to this.
One laboratory worksheet question for the second intervention topic asked what nurses can tell from urine testing. This time, more of the students showed awareness of the link between their science learning and their future professional practice. Table 6 shows the pattern of responses, with most answers conveying a sense of purpose behind the action, albeit often not explicitly linked to what a nurse could do. Some answers could be assigned multiple codes as they were longer and more comprehensive.
| Type of response (N=104) | % giving this type of response |
|---|---|
| General answer (to see what’s wrong/to see if it is normal) | 72 |
| Mentions diagnostic possibilities (e.g., to check for abnormalities, signs of infection, diabetes) | 40 |
| Mention of types of empirical evidence that can be gained (e.g., colour, smell, presence of blood, ketones or drugs, pH.) | 47 |
| Makes some specific link to their own role as a nurse | 39 |
By contrast with the earlier topic, there were many more mentions of the specific types of empirical information that could be gained from urine testing, and of the diagnostic potential of this information. In about a third of the linked responses the answer was more explicit about what a nurse might actually do next—for example, ameliorating dehydration by providing more water, or undertaking further testing.
Issues and challenges
Content reduction
Some of the Māori students in Cohort 21, who were taking the module for the second time, were aware of the ways in which teaching staff had made significant changes to the lectures and associated resources through content reduction, and how these changes assisted their learning in 2007 compared to 2006. Three of these students took part in a focus group after the intervention topics for BN were completed. They noted:
The method of delivery is different—slightly but different—simplified it and more diagrams, outcomes are clearer, simple wording rather than scientific jargon, we understand it better, the focus is better.
In the past the tutors were so enthusiastic about their subject that they just gave us too much information, 2006—information overload; they gave you the readings but you did not know what to take out of it.
When they carried out their self-review, the science tutors also noted that content reduction had worked well and had played an important part in establishing relevance and maintaining the interest of students. The stories captured students’ curiosity, but the questions the stories generated sometimes took up more time than content reduction had freed up, resulting in the tutors feeling they were “rushing a bit at the end” of some lectures. One tutor commented that:
Student interest was higher than previous years. They [the stories] made it more interesting for me and for the students. I enjoyed delivering the content, with more people asking questions and having more response to comments. Also the number of students attending remained high throughout the series of lectures. The increased interest is sensed from the front of the lecture theatre.
The science tutors thought that most BN students had learnt the essential ideas of the lectures, as evidenced by the comments on the “tickets out of class” and by the BM students being able to answer all of the questions relating to the story. However they did raise issues of a potential halo effect. As one commented, “the energy associated with the research means that we are doing a better job of putting together the whole package of lectures, labs and tutorials plus formative tests.” One tutor also expressed concern that, as a result of content reduction, key concepts which linked first-year content to second year were being lost and not covered.
Notwithstanding the tutors’ content reduction of lecture materials, discussions in the SGID groups revealed that students saw the amount of information in lectures, along with the many scientific words and their definitions, as hindering their learning. They said the speed of lectures was too fast and there was not enough time to process their thinking. Suggestions for improvement in the SETMAP similarly mentioned changing the pace of lectures. They were seen as too rushed, and students felt there was no time to understand information.
With these challenges in mind, the tutors were thinking ahead to the remaining first-year science modules. Having used this narrative approach once, they could see ways to reorder and refine the strategy on a second occasion. For example, one of the tutors said “stories are cool, but all three at the start of the lecture would be better. I would rather spend more time going over the stories scenarios again—I need to reduce content even further, there is still plenty to discuss in relation to the stories which reinforces the main points of the lecture.”
Designing effective narratives
Reflection on the impact of the narratives shaped for the two science topics in the nursing module suggested a design principle of importance for future modules.
The CVS topic was taught first, and the stories shaped for this unit cued students to situations where medical help might need to be sought if this body system malfunctions. Such situations were likely to be familiar to students, and introduced suggestions of patho physiology to the module. (This initial programme has historically been intended to teach ‘normal’ system functioning in the belief that it is better to understand healthy bodies before addressing illness and disease and is now being reviewed). These stories differed from those in the second unit in one subtle but, as it turned out, powerful way. The heart stories were resolved, if compact, narratives. Something happened and the consequence was medical intervention. These stories gave a contextual illustration of the relevance of the intended conceptual learning, but the context of the story did not link in any necessary way to the concepts being taught. The “content” of the lecture could proceed as planned, with or without the narrative. Rather like attractive wrapping on sweet treats, the heart stories were designed to attract students to want to know more. However, questions posed by some students at the end of the lectures showed that the purpose the stories served was not necessarily clear, and for some they added to confusion rather than helping build links between theory and prospective practice.
Lessons learned from this first attempt ensured that narratives shaped for the second unit opened up questions of importance for conceptual understanding, in a context where medical intervention could be implicated. Here contexts and concepts were more interwoven, and the story invited discussion that would draw students into a more personal response to the intended learning. The next example, used at the very start of the unit, illustrates this difference:
In January 2007 Jennifer Strange, a 28-year-old woman from California was found dead in her home after trying to win a Nintendo Wii game console in a radio station’s ‘Hold Your Wee for a Wii’ contest, which involved drinking large quantities of water without urinating. The coroner blamed her death on drinking too much water. (http://www.nbc4.tv/news/10761800/detail.html)
Do you believe the water killed her? Could you die from drinking too much water? What would the cause of death be? Was there something wrong with her kidneys? How much water is it safe to drink? (Wintec, 2007b)
Discussion in response to the story and its accompanying questions was lively and easy to align with the “content” of the session to follow. Further stories were variations on this theme (for example, a top athlete becoming disoriented when dehydrated during a long distance race), and these added more dimensions to the mystery of how something as seemingly innocuous as water could have such a profound effect on body functioning, and how medical interventions, based on a biological understanding of what was going wrong, could help. These narratives, with their element of surprise and unanswered questions, invited students to draw on their emergent understandings of the excretory system as the unit unfolded, and they were revisited as new concepts were added. Thus the design principle here suggests that effective narratives position both context and concepts as integral to the intended learning. Here the narrative carries links in both directions, potentially creating the intended bridge between theory and practice.
In a somewhat different manner, this principle was also implicated in the less successful midwifery intervention. For reasons discussed earlier, this did not unfold as originally planned. One narrative served the somewhat awkward function of creating a segue within a lesson, from midwifery concerns grounded in the social sciences to the physical science of lactation. This happened at the point of the lecture where the science tutor took over from the midwifery tutor. The science tutor felt that while she made links from the narrative into the science of lactation, the students did not see these links. Essays subsequently written by this group of students confirmed that they had not made the link between the intended science learning and the midwifery role. Most students did not appear to see the science they had been taught as having any direct role to play in informing their decision-making or communication with their clients.
As with the confusion for BN students created by the additional laboratory worksheet questions, midwifery students may have been “thrown” as to how to correctly interpret and answer the essay with the additional criterion where they were to describe the science and rationale underlying the process of lactation and breastfeeding. There was also tension between the “story form” of the experience of the breastfeeding woman and the discussion of the underlying science of lactation. The structure of the assignment may have hindered the introduction of the science. It has been noted that in future the essay may need to be structured in a different way, and that the essay question may need a little work. The essay question was set at the end of 2006, and our understanding of what we were trying to achieve was not as developed then as it had become by midway through 2007.
Other challenges for the tutors
Early feedback with the TOC was discouraging for the science tutors. The questions students asked highlighted gaps in understandings—gaps of which the tutors may have been less aware in previous years. This was understandably disconcerting, and at first the tutors felt they were doing a worse job than previously. A breakthrough came when they realised that, rather than reiterating the intended learning in response to questions, they needed to engage with the actual questions asked. This quickly led them to a better understanding of some stumbling blocks, and they began to gain a feel for ways of linking theory to practice in ways that prompted productive and engaging questions.
There are issues of scalability and sustainability. Developing the narratives took a lot of effort, but was seen as worthwhile. For example, “it was a pain having to rewrite the lecture but it is something that I will continue to use. In principle it went okay. I think that it is worth my while. It takes more time but the more you do it the easier it becomes and it is worthwhile for the students.” Despite the effort involved, one of the tutors intended to recommend the approach to other tutors in a new degree programme Wintec was developing.
Another issue raised by science tutors related to the timing and alignment of curriculum content in the midwifery intervention. When teaching about the process of lactation, which is influenced by hormones, tutors realised that students did not know what hormones were. Next year the tutors plan to move the endocrine system topic in the “introduction to science” module forward in the semester, so that by the time the lactation and breastfeeding module occurs, students will have had access to the relevant background knowledge about hormones. One tutor commented that “as we implement research ideas more widely we need to check the curriculum to keep the changes in alignment and also monitor the impact on other related classes”.
Rethinking assessment
End-of-year summative test results for 2006 and 2007 were compared for five topics taught during the year, including the two intervention topics. Some of the questions asked were slightly different in 2007, yet similar enough to be compared. Despite the considerable efforts of the tutors, assessment results in 2007 were similar to those for 2006, and there was no obvious improvement. The overall failure rate of students in 2007 remained around 30 percent.
Discussing why this might be, the science tutors identified a mismatch between the intent of the intervention and the assessment tools. They felt they needed to revamp the multiple-choice questions because their general tenor was still about remembering detail, whereas the research intervention focused on the application of science to practice situations. Interestingly, the students themselves did not seem to see this mismatch. When completing the SETMAP exercise, approximately three-quarters of the BN students and most of the TMO students agreed/strongly agreed that “assessment requirements relate closely to the topics and content of the module”.
The science tutors wondered if the change in students’ results would be more noticeable in Year Two of the BN. The science tutors reported in 2008 that the failure rate for the first science test (on the cardiovascular system) for second year students (Year One participants in 2007) had reduced from approximately 30 percent to 15 percent. Half of the students that failed did so by only one or two marks. This could be attributed to different variables. Participation in the intervention topics may well have contributed to the reduction in the failure rate.
Cohort 21 provided an opportunity to see if students who had undertaken some clinical practice in 2006 and were repeating science modules in 2007 made links between the theory they were learning and their previous clinical practice. Disappointingly, we had minimal participation from this group in all of the data-collection exercises. Cohort 21 students completed an additional question on the TOC for the laboratory session that asked about links between the learning activities and their clinical experience the previous year. For the CVS laboratory session, 16 students completed the TOC, and nine attempted the additional question. For the renal laboratory session, only nine students completed the TOC, with six attempting the additional question. In each case, like their first-year peers, Cohort 21 students were more likely to recap the main theme from the laboratory than to relate the content to clinical practice. However two students in the cardiac laboratory commented:
What a ‘swish-dub’ noise means to a patients condition. Blood pressure relates to the heart rate. I can identify the chambers of the heart & their functions.
Understanding blood flow directions & why we test vital signs so often & the need …
Similarly, for the renal laboratory two students commented:
Identify normal urine from abnormal urine
Ecur test used very much to detect UTI [Urinary Tract Infection] in the older person at the rest home.
Even though these students had undertaken clinical practice, it seemed most of them still struggled to make links between what they had learnt in laboratories and their own clinical practice experience—at least in terms of links they could write down. When asked what had hindered their learning in the intervention topics in 2007 in comparison to 2006, these students reported that knowing what written language to use to describe something in assessment was difficult.
Getting stuck on words when writing the short answers hinders me. In the test today, asked to ‘describe’ … I found that I had studied it but I lacked the words to explain the images in my head. I got stuck—I am a perfectionist, the explanations in writing are still hindering me this year, they hindered my last year, trying to grasp the language—how to construct my sentences—because I am more visual. No words in my head—just images. I lack the tools to explain the images.
Just to get the questions—we work in a group. Perhaps if we took a topic and had to explain it in words—that may be better. Short answer questions I have to practise. You have to phrase the diagram in words, in short answer.
Congruent with the learning challenge implicated here, when students were asked in the focus groups to think about whether clinical practice they had completed in 2006 had assisted their learning of the repeated CVS and renal intervention topics in 2007, they were able to make clear links as they talked. The three students who took part did say they were better able to relate to the information in lectures and laboratories as a result of having had some clinical practice:
One aspect I found really useful was using the sphygmomanometer [equipment for taking blood pressure]. We had a whānau day—we assisted with doing blood pressure. … I could relate what I was doing to this year. I went through the clinical last year and I didn’t quite grasp it but this year going through the CVS again and just getting my sphygmomanometer out and looking at the different parts and saying what do I need from there? … Because I am doing it again it helped me understand it better, it helped with the CVS understanding.
It does instil a sense of confidence to learn new things that are in the CVS for me. I can relate my learning to my practical side. The first time around I could never understand it— could not understand how it all works. Second time drew a lot of pictures and compartmentalised the heart, reading and re-reading and to relate it to my practical—the sphygmomanometer, how we understand the CVS.
It sinks in a wee bit, starting to be aware of odours blood cretins in the urine etc. Before the object was to get it cleaned up and make sure that the resident was in comfort but now you are thinking. That’s only—the more knowledge the better it is.
Such responses suggest that the apparent lack of links in written work were more about the mode of assessment than a lack of actual connections. This is something the research team would like to explore further in 2008.
Summary of conflicting findings
The students provided positive feedback overall regarding teaching methods and resources. Only Cohort 21 students were able to comment on the intervention topics prior to and after content reduction, and they agreed that the strategies tried out were helpful. There was evidence of increased motivation and engagement of students compared to previous years, but there was no clear evidence of improvement in the summative test results. Nevertheless, the science tutors were planning to carry the principles of content reduction and inclusion of narratives into other science modules and modules they taught in other areas, because they were convinced of the improvement in student engagement and learning. An emergent focus was to address assessment practice, so that it better reflected the intent of the innovation and the reduction of fine detail in the module content.
5. How the project contributed to building capability and capacity
Relationships/partnership
This project involved two sets of collaborations, one nested inside the other. In the first instance, the project was a collaboration between staff from four different areas at Wintec: a researcher from the Research Office, a professional education tutor from the School of Education, two science tutors from the School of Science and Primary Industries, and a nursing tutor from the School of Health. This team then worked with researchers from NZCER.
With so many different perspectives being brought together, relationships and partnerships have been fundamental to the success of our research. Based on their previous projects, the two experienced researchers from NZCER reinforced the importance of getting the relationships right, and having a shared understanding of the research aims even before the funding was secured. Harmonious relationships foster enjoyment of the research process and increase the likelihood of successful completion of the project.
A two-way interchange allows for the knowledge of tutors (both theoretical and practical) and the knowledge of researchers (again both theoretical and practical) to be brought together as new ideas are tried out and new meanings forged. It is not the case that science education theory was applied unidirectionally to teaching science in health programmes. Rather, the project aimed to weave multiple aspects of theory and practice together, without losing the influence of either. This paralleled the aim of the research, which was to help students make more meaningful theory–practice links, and respected the potential of each to inform the other (Mackler, 2005). Having enough time, both in regular meetings and in all-day workshops with the external partner, has been critical to maintaining relationships, for talking through our ideas, and establishing shared understanding.
Trust and agreement about directions, priorities, and values can be especially important when the going gets tough, and practical or conceptual challenges have to be met and overcome. Such challenges may be encountered unequally by different members of the team. In this project, for example, the science tutors bore the brunt of the uncertainties that are inevitably associated with changing personal pedagogical practice, and they did so “in the spotlight”, given the interest of the whole team in the outcomes of their experimentation. This took considerable courage, commitment, and trust.
Building capability
Some of the research team had had limited experience as qualitative researchers, particularly the science tutors who were used to researching in the quantitative paradigm. When undertaking data collection or analysis tasks we tended to pair up a team member with limited qualitative experience with another with more experience of working in this paradigm; for example, when conducting focus groups for Phase One. Both science practitioners now have an understanding of and experience of undertaking qualitative social science research as practitioner-researchers. Having an external senior research partner mentor also facilitated this learning. One indicator of the success of this process was that the mentor was invited by one of the science tutors to be a Visiting Scholar to the School of Science and Primary Industries, presenting two workshops about “effective teaching in the knowledge era” to staff who would be involved with the teaching of the new Bachelor of Technology at Wintec. In this context, the lines between being a teacher and being a researcher, between theory and practice, were thoroughly blurred.
Footnotes
- This is the shortened working title for the research project. ↑
- EBP = Evidence Based Practice ↑
- For the purposes of this paper, the term new graduate is used to describe the working practices of recently graduated midwives and nurses working in hospitals, and midwives working as Lead Maternity Carers. ↑
- This is a confidential process in which consensus about what helps or hinders learning is debated, along with suggestions for improvement. SGIDs were completed for both intervention topics (involving 117 students for the CVS topic and 108 for the renal topic). ↑
- This comprised 17 Likert Scale questions, selected by the tutors from an established item bank; written feedback about aspects of the module that were done well; aspects in need of improvement; and any other comments. SETMAP data was gathered from BN students (n=88) in tutorial groups and from BN students who were enrolled in the TMO support network for Mäori students (n=13).↑
References
Aikenhead, G. (1996). Science education: Border crossing into the subculture of science. Studies in Science Education, 27, 1–52.
Aikenhead, G. (2005). Science-based occupations and the science curriculum: Concepts of evidence. Science Education, 89, 242–275.
American Association for the Advancement of Science. (2001). Unburdening the curriculum. In Designs for Science Literacy. Retrieved 15 November 2006, from http://www.project2061.org/publications/designs/ch7.pdf
Angelo, T. A., & Cross, K. P. (1993). Class room assessment techniques: A handbook for college teachers (2nd ed.). San Francisco: Jossey Bass.
Benner, P. (2001). From novice to expert: Excellence and power in clinical nursing practice: Commemorative edition. Upper Saddle River, NJ: Prentice Hall Health.
Bruner, J. (1986). Actual minds, possible worlds. Cambridge, MA: Harvard University Press.
Chin, P., Munby, H., Hutchinson, N., Taylor, J., & Clark, F. (2004). Where’s the science? Understanding the form and function of workplace science. In E. Scanlon, P. Murphy, J. Thomas, & E. Whitelegg (Eds.), Reconsidering Science Learning. London: RoutledgeFalmer.
Gibson, K., Stewart, J., Christie, D., Dannenfeldt, G., Anderson, V., McHaffie, J., et al. (2005). Executive summary of the scoping project for addressing obstacles to success: Completion and retention issues for Māori students in science modules in applied health programmes. Hamilton: Faculty of Health, Arts, & Social Sciences, Wintec.
Gibson-van Marrewijk, K. (2005). Executive summary of the abridged report of the retention strategies for Māori students studying at Waikato Institute of Technology research project. Hamilton: Faculty of Health, Arts, & Social Sciences, Wintec.
Gilbert, J., Hipkins, R., & Cooper, G. (2005, June). Faction or fiction: Using narrative pedagogy in school science education. Paper presented at the Redesigning Pedagogy: Research, Policy, Practice conference, Nanyang University Institute of Education, Singapore.
Mackler, S. (2005, December). The company we keep: In search of a more genuine partnership between mind and body, theory and practice, scholarship and life. Available from www.tcrecord.org
Nutley, S., Walter, I., & Davies, H. (2003). From knowing to doing: A framework for understanding the evidence-into-practice agenda. Evaluation, 9(2), 125–148.
Statistics New Zealand. (2006). 2006 Census: Quickstats about Waikato Region. Retrieved 31 January 2008, from www.stats.govt.nz/census/census-outputs/quickstats/snapshotplace2.htm Wintec. (2004). Arion database. Hamilton: Author.
Wintec. (2007a) Tihei mauri ora. Retrieved 21 February 2008, from http://www.wintec.ac.nz/ index.asp?pageID=2145826978
Wintec. (2007b). Body fluids [Lecture handout for SCBN524]. Hamilton: Author.
Wintec. (2007c). Breastfeeding and lactation module [Lecture handout for science NUM0203]. Hamilton: Author.
Acknowledgements
We would like to acknowledge all the participants who graciously took part, and the TLRI fund for enabling us to undertake this research.
During Phase Two of the project, Dr Margaret Duff, one of the researcher-practitioners, left Wintec and was unable to continue in her role as a research team member. We would like to acknowledge her valuable input into the research project to that point.
We would also like to acknowledge Dr Jane Gilbert, New Zealand Council for Educational Research (NZCER), for her support during the establishment of this project, and for her recognition of the ground work needed for our working relationships and shared vision for the research, which needed to be further developed before applying to the TLRI fund in 2005.